48 Year old male with chief complaints of shortness of breath
*NOTE- This is an ongoing case, this E-log will be updated as and when we find new information.
HISTORY OF PRESENTING ILLNESS
The patient was apparently asymptomatic
2 years back, on routine examinations, he was found to have a deranged RFT, a diagnosis of Chronic renal failure was made and conservative, symptomatic treatment for the same was done.
7 months back, the patient had chest pain, for which he visited a hospital where he was said to be having heart failure, an angiogram was done after which he was normal.
2 months back, the patient had Shortness of breath for which he went to a hospital and was given symptomatic treatment.
He was asymptomatic for those 2 months
One week back, he again had shortness of breath grade - II (from the past 1 week ) which progressed to grade III-IV in the past 4- 5 days, orthopnoea and bendopnoea were present.
HISTORY OF PAST ILLNESS
Known case of
- Diabetes Mellitus from the past 7 years
- Hypertension from the past 7 years
- Chronic renal failure was diagnosed 2 years back
- Heart Failure 7 months back, angiogram was done
No History of -
- CAD,ASTHMA,TB
DRUG HISTORY
Till the day of admission, the patient was using Tab. Shelcal
PERSONAL HISTORY
- Married
- Occupation - construction worker
- Appetite - Normal
- Diet-Non vegetarian
- Bowel Movements- Irregular
- Micturation - Normal
- The patient is a known alcoholic for the past 25 years, and he stopped consuming alcohol 3 years back.
FAMILY HISTORY
- No relevant family history
GENERAL EXAMINATION
- The patient is conscious, coherent.
- Edema of feet present
- Absence of Cyanosis, Pallor, Icterus, Lymphadenopathy, clubbing.
VITALS
- Temperature - Afebrile
- Respiratory rate - 18 beats per minute
- Blood Pressure - 100/80 mmHg
- SPO2- 98 percent
CVS EXAMINATION
- S1, S2 heard
- No Murmurs or thrills
RESPIRATORY SYSTEM EXAMINATION
- Dyspnoea - present
- Wheeze - Absent
PER ABDOMEN
- No tenderness, palpable mass, Free fluid
- Non-palpebral spleen and liver
- Bowel sounds heard
CNS EXAMINATION
- The patient is conscious
- He has normal speech
- No neck stiffness, kerning sign
- Cranial nerves - Normal
- Motor and Sensory system normal
- Glasgow scale - 15/15
- Fingernose incoordination, Knee heel Incoordination - Absent
- Normal gait
INVESTIGATIONS -
1.Fasting blood sugar -Elevated



4. Erythrocyte sedimentation rate-Elevated

5.Complete blood Picture- Hb lower than normal

6.ABG

7.Liver Function Test

7. Lipid Profile

8.USG report

9. Renal Function Test
(10/7/2021)

(14/7 2021)

10.2 D echo

11.ECG

INVESTIGATIONS - 20th July 2021
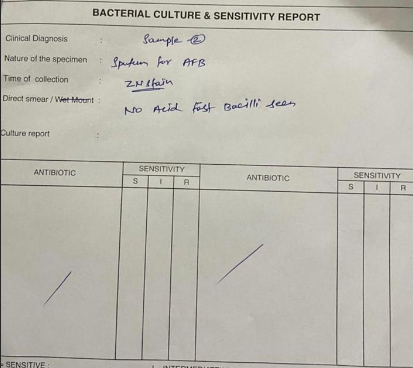
1. AFB CULTURE AND SENSITIVITY REPORT -
NEGATIVE- 

2. PULMONARY FUNCTION TEST - 20th July 2021
Findings-
Pre Medication findings
1. Early small airway obstructions as FEF25-75 % Pred or PEFR % Pred <70
2.Spirometry within normal limits as (FEV1/FVC) % Pred> 95 and FVC% Pred >80
Post Medication Findings
3. Mild restriction as (FEV1/FVC) % Pred >95 and FVC % <80

PROVISIONAL DIAGNOSIS - HFrEF secondary to CAD; CRF
DIAGNOSIS -
ACUTE ON CHRONIC LVF
HFrEF SECONDARY TO CAD
CKD- STAGE 4
RENOCARDIAC 4
TREATMENT - DAY 1
1. TAB. BISOPROLOL 5mg OD
2.TAB. NITROHART 20/37.5mg 1/2 T/D
3.TAB NICARDIA XL 30mg OD
4.TAB. GLICIAZIDE 80mg BD
5.TAB. NODOSIS 500 mg TD
6.Cap. BIO-D3 OD
7.Cap. GEMSOLINE OD
8.TAB. ECOSPRIN-AV 150/20mg OD
9.TAB.LASIX 40mg BD
10. SYP. LACTULOSE 15ml
TREATMENT DAY 2
- FLUID RESTRICTION <1.5 L /DAY
- SALT RESTRICTION <2 G DAY
- TAB BISOPROLOL 5MG OD
- TAB NICARDIA XL 30mg OD
- TAB. GLICIAZIDE 80mg BD
- TAB. NODOSIS 500 mg TD
- Cap. BIO-D3 OD
- Cap. GEMSOLINE OD
- TAB. ECOSPRIN-AV 150/20mg OD
- TAB.LASIX 40mg BD
- SYP. LACTULOSE 15ml
TREATMENT DAY 3 -
- FLUID RESTRICTION <1.5 L / DAY
- SALT RESTRICTION <2 G /DAY
- TAB BISOPROLOL 5MG OD
- TAB GLICIAZIDE 80 MG BD
- TAB NODOSIS 500 MG TID
- CAP BIO - D3 OD
- CAP GEMSOLINE
- TAB. ECOSPRIN-AV 150/20mg OD
- TAB.LASIX 40mg BD
- TAB HYDALIZINE 25 MG PO /TID
- SYP CREMMAFIN PLUS 15 ML / TID
SUMMARY
-
This is the case of a 48 year old male who presented with chief complaints of shortness of breath , the patient has a history of chronic renal failure 2 years back and heart failure seven months back . The patient has Diabetes mellitus and Hypertension from the past 7 years , on examination we found out that the blood glucose was higher than normal , symptomatic treatment was done for it , renal function test was deranged and atrial flutter / tachycardia , with rapid ventricular response, widespread T wave abnormality was seen in the ECG
A provisional diagnosis of Heart Failure with reduced ejection fraction secondary to CAD was made, with CKD . Acid fast bacterial culture was done , the report was negetive ,as a result the pulmonary function test was done , on the basis of which the following diagnosis was made
ACUTE ON CHRONIC LVF
HFrEF SECONDARY TO CAD
CKD- STAGE 4
RENOCARDIAC 4
LINKS-
Beta-blockers and renin-angiotensin system inhibitors have yielded promising results in patients with HFrEF associated with advanced kidney disease .
2. Heart failure in patients with chronic kidney disease: a systematic integrative review
Liviu Segall, Ionut Nistor, Adrian Covic, "Heart Failure in Patients with Chronic Kidney Disease: A Systematic Integrative Review", BioMed Research International, vol. 2014, Article ID 937398, 21 pages, 2014. https://doi.org/10.1155/2014/937398Patient, Problem: Adults with a primary diagnosis of CKD and HF
Intervention: HF treatment was defined as any formal means taken to improve the symptoms of heart failure
Comparison: 1439 Patients were compared, and 23 articles were hand-searched.
Outcomes: Control of fluid overload, use of beta-blockers and angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, and optimization of dialysis appear to be the most important methods to treat patients with HF in CKD and ESRD patients

Comments
Post a Comment