Case of a 68 year old female with vomitting and loose stools
This is the case of a 68-year-old female who presented to the causality with chief complaints of
- Vomiting since 2 days
- Loose Stools since 2 days
History of Presenting Illness
The patient was apparently asymptomatic 2 days ago
2 Days ago, at 6 PM, the patient had an abrupt onset episode of vomiting. The vomitus was not bile stained, contained the food particles eaten previously, was non-blood stained, and was not associated with retching, and was non-projectile. Since the first episode, the patient has had about 12 such episodes in a duration of 2 days. The last meal eaten was on the day of the first episode - Fish saalan. It was also consumed by other family members who showed no symptoms. Since then, the patient has not eaten any other meal and describes vomiting the water she has intaken.
With the onset of vomiting, the patient had episodes of loose stools. The loose stools were green in colour, foul-smelling with no blood stains or mucous present. The patient has had 8 such episodes of loose stools in 2 days. There is presence of tenesmus. There is presence of acute pain abdomen since these symptoms.
The associated symptoms include fever (which was not checked at the time of onset, so the degree is not known) not associated with chill and rigour. The patient visited a doctor and was treated for the fever, but the symptoms were not relieved.
Yesterday night, the patient developed hypotension and was rushed to the casualty.
Past History
The patient had a history of bowel perforation 14 years ago, for which she underwent surgery and blood transfusions.
Soon after the surgery, the patient developed chikungunya and was treated for the same.
10 years ago, first experienced pain in her metacarpal joints, for which she was given steroids.
The patient had one such episode of vomiting and loose stools 4 months back, which resolved on its own.
The patient is not a known case of Diabetes Mellitus, Hypertension, Tuberculosis, Epilepsy, and Cardiovascular disease.
Family History
The patient's Father also has similar joint deformities
Personal History
Diet: Mixed
Appetite: Reduced
Usually, the patient's food habits look like
- Consumes tea and biscuits at 6 AM in the morning
- Followed by lunch at 12 / 1 PM
- At night, the patient usually does not consume food.
Bowel Movements: Regular previously, till episodes of loose stools
Bladder movements: Normal
Addictions: The patient consumes Pan For 40 years 3-4 times a day.
General Examination
The patient is conscious, coherent, and oriented to time place and person.
The patient is well-built and well-nourished.
Pallor - absent

Icterus- absent

Cyanosis - absent


Clubing , Koilonychia - absent


Lymphadenopathy - Absent
Oedema - Absent

Per Abdomen
Inspection
Shape - Distended

Flanks - Full

Umbilicus- Inverted
Skin - Scar from previous surgery present in the midline approximately 30 cm
Dilated veins - absent
Visible gastric paralysis absent
Palpation
Tenderness elicited in all 9 quadrants
No local rise of temperature
Spleen - Non-palpable
Investigations
2 D echo


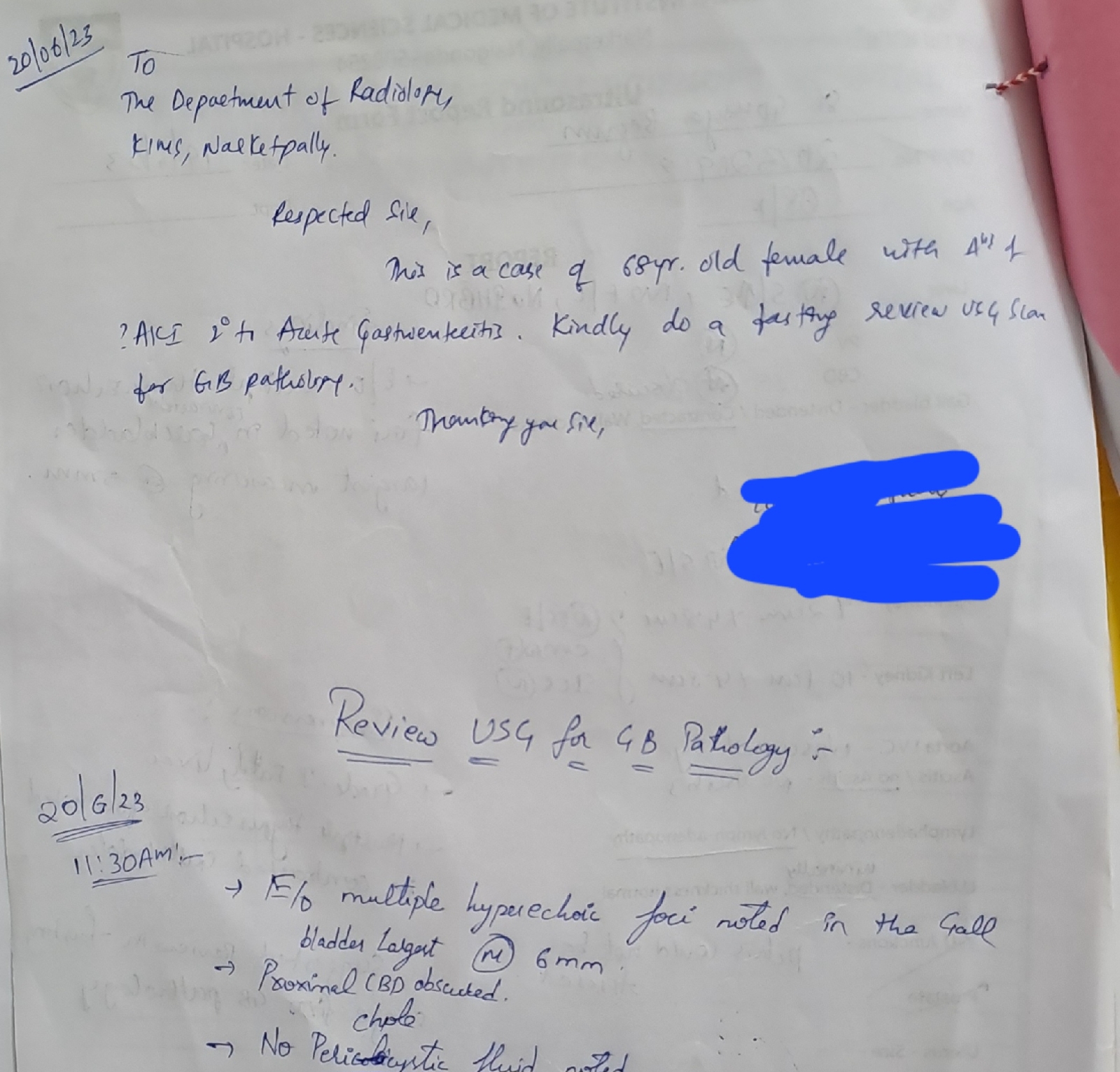
Ultrasonography

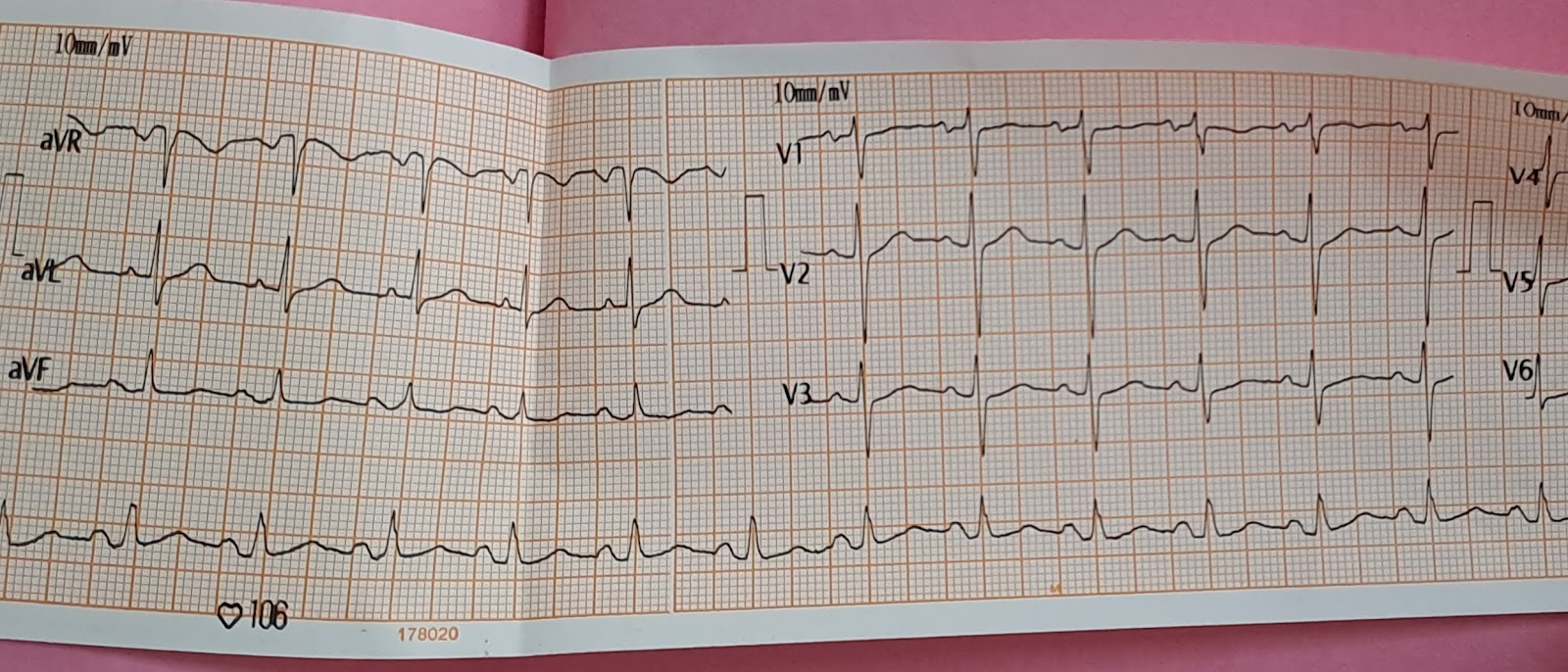
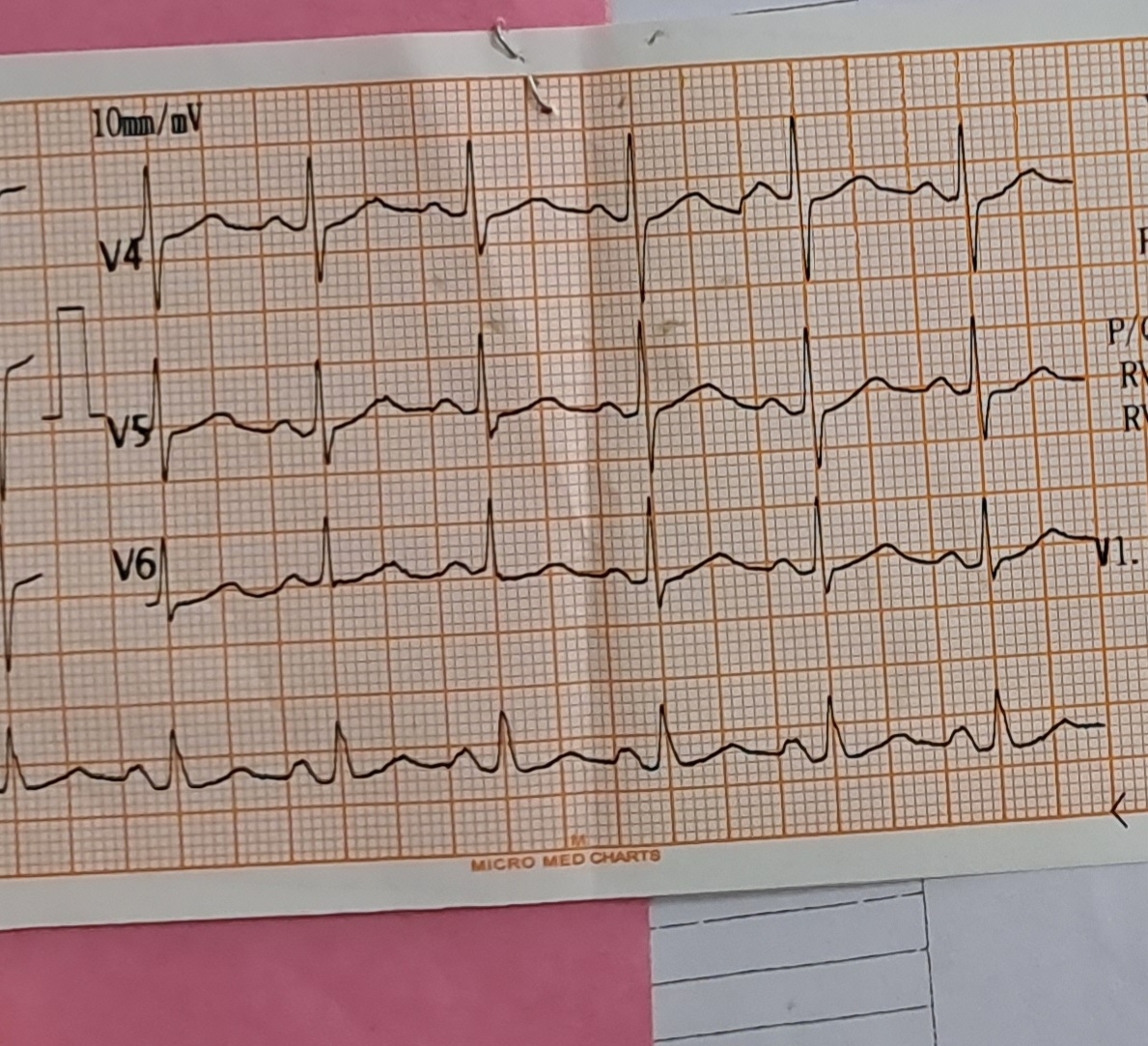
ECG

Diagnosis
? Acute gastroenteritis
History based case discussion


Comments
Post a Comment