Case of an 82 year old female with painful bilateral swelling of the knee joint and lower limb below the knee
This case was created under the guidance of Dr, Raveen sir
This is the case of an 82-year-old female who presented to the hospital with chief complaints of
- Pain in the lower limbs since 2 days, bilaterally
- Fever since 2 days
- Swelling in the lower limb, bilaterally since 2 days
History of Presenting Illness
The patient was apparently asymptomatic 6 months ago.
6 months ago, the patient experienced a pricking type of joint pain while climbing the stairs, it was pricking in nature, and the patient could carry out her daily activities without hindrance.
On 25th May 2023, After waking up at 5 AM, the patient could not lift her legs from the bed. The patient explains that she had to drag her feet to the washroom.
In a matter of three days, the patient developed a sudden onset of pain. The pain was pricking in character, and continuous. present bilaterally in the lower limbs at and below the level of the knee. It aggravated on walking and relieved at rest.
The pain was associated with swelling of the lower limb at and below the level of the knee joint, bilaterally. It was associated with redness over the limbs.
The patient also experienced high-grade fever, which was continuous, and . not associated with chills and rigour. She also experienced generalised body pain and malaise.
2 Days later, the patient visited a doctor and was prescribed medications. The symptoms reduced after the consumption of medicines.
One week later, there was a sudden increase in pain and swelling similar to the last episode. There was also a rise in fever up to 104 degrees Fahrenheit.
The patient came to our hospital and was given, NSAIDS, paracetamol,normal saline and antibiotics. This resulted in a reduction of symptoms, and the patient was discharged.
2 Days later, the patient developed the same constitution of symptoms again and came to our hospital.

Past History and treatment history
The patient is a known case of hypertension since 10 years and has been on Telmisartan and Amlodipine since then.
10 years ago, the patient had a history of trauma, that led to a fracture of the ulna.
8 Months ago, the patient had a syncopal attack and was started on low-dose aspirin as a prophylactic measure.
The patient is not a known case of Diabetes Mellitus, Tuberculosis, CAD, or Epilepsy.
The patient consumed NSAIDs when she experienced pain.
She was prescribed Diethyl Carbamazine, on her first visit to the doctor since 15 days.
She was prescribed amoxicillin seven days ago.
Family History
Brother and sister have asthma.
Personal History
Appetite: reduced since yesterday
Diet: Vegetarian
Sleep: The patient consumes alprazolam (on prescription) as she has difficulty falling asleep.
Bladder: 9 months ago, the patient had oliguria, since the onset of fever, she has increased the frequency and urgency of micturition.
Bowel Movements: Normal
Addictions: None
Allergies: none.
General Examination
The patient is conscious, coherent, and oriented to time, place and person.
The patient is moderately built and moderately nourished.
Vitals :
- Pulse - 94 beats per minute
- RR- 16 cycles per minute
- Temperature: Afebrile
-Blood Pressure- 120/70 mmHg
Pallor - Present

Icterus - absent

Cyanosis - Absent


Clubbing - Absent

Koilonychia - absent
Lymphadenopathy - Absent
Oedema -present

Peripheral pulsations were felt in the dorsalis pedis, anterior and posterior tibial arteries, and radial arteries.
Examination of the Musculoskeletal System
Inspection findings -
Bilateral swelling of the lower limbs, at and below the level of the knee joint. More prominent on the right than the left.
Right, Limb Fixed flexion deformity seen at the knee joint.
Left lower limb, ability to flex knee present.
No scars, sinus, erythema or rashes



Palpatory Findings
Local rise of temperature present bilaterally on the knee joint
Palpable swelling is present on the right and left knee, and ankle with mild oedema in her lower limbs , associated with tenderness, in the suprapatellar bursa
Patellar tap is positive bilaterally.
Join Line tenderness observed.
absence of lower limb shortening.
Range Of Motion
Inability to flex the left lower limb.
Upper limb Findings
Inspection
-4th metacarpal hyperextended. In the right hand .

Palpatory
- no tenderness
Range of motion
- reduced.
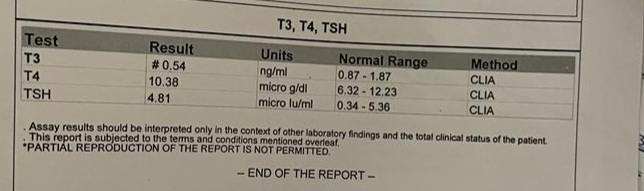
Investigations






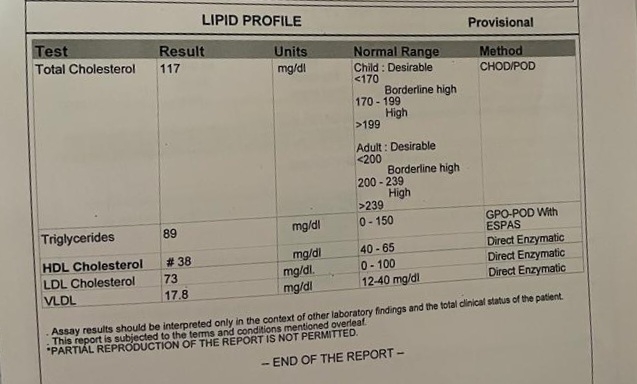






? Bursitis
? Osteoarthritis
ADMISSION 3
20 days after the second discharge, the patient presented to the causality again with chief complaints of Fever and generalised body weakness , both since one day.
History of Present Illness
The patient was apparently asymptomatic 1 Day ago
1 day ago, the patient experienced fever in the evening. Which wassudden onset continuous , high grade (104 degree F). It increased at night afterwhich the patient was brought to the casualty. It was relived on taking paracetamol (Dolo 650). No aggravating factors , not associated with chills and rigour.
Since the onset of fever, the patient also experinced generalised body weakness.Which was gradual in onset and progressive in nature. And still persists. The patient describes the inability to get up from the bed and a feeling of heaviness in the legs.




Treatment admission 3 ;
Neomol, telmisartan, paracetamol, orofer,Ultracet, shelcal
Diagnosis :
Pyrexia with polyarthralgia with iron deficiency anemia


Comments
Post a Comment